The Role of Anesthesiologist in Weight Surgery
Published June 24, 2026

The Role of Anesthesiologist in Weight Surgery
The anesthesiologist in weight loss surgery is a medical doctor who manages every phase of anesthesia to protect patients with obesity from serious physiological risks. This is not a supporting role. Bariatric anesthesiology requires specialized training because obesity changes how the body responds to drugs, breathing, and surgical stress in ways that standard protocols cannot address. Understanding the role of anesthesiologist in weight surgery helps you ask better questions, prepare more thoroughly, and choose a surgical team that treats anesthesia as the safety-critical specialty it is.
What are the unique anesthetic challenges in weight loss surgery?
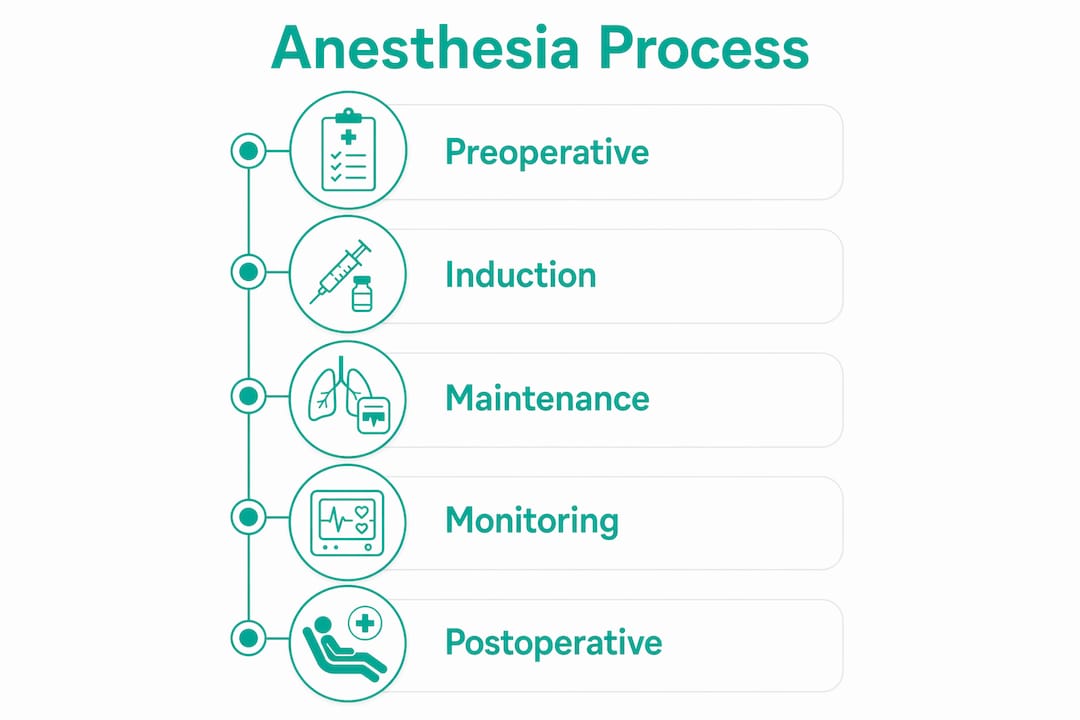
Obesity creates physiological conditions that make anesthesia significantly more complex than in average-weight patients. The integrated three-phase approach of preoperative, intraoperative, and postoperative anesthetic management exists precisely because these challenges span the entire surgical experience.
The two most dangerous factors are lung function and airway access. Obese patients experience a 30–50% reduction in functional residual lung capacity. That means the lungs hold less reserve oxygen, and patients can desaturate to dangerous levels in under three minutes during apnea.

Airway management compounds this risk. Difficult mask ventilation is 3–5 times more likely in obese patients than in the general surgical population. The combination of a shorter neck, excess soft tissue, and reduced lung reserve creates a narrow window for safe intubation.
Obstructive sleep apnea (OSA) is present in 40–70% of morbidly obese patients. OSA blunts the body's normal response to low oxygen, which means patients may not signal distress the way non-OSA patients do. An anesthesiologist who does not screen for OSA before surgery is missing one of the most predictable risk factors in bariatric care.
Drug dosing adds another layer of complexity:
- Induction agents like propofol are dosed on ideal body weight, not total body weight, to prevent overdose.
- Maintenance dosing of propofol is capped at a maximum of 4 mg/kg/hr based on total body weight to avoid Propofol Infusion Syndrome, a rare but life-threatening complication.
- Opioids and muscle relaxants require separate dosing calculations because fat tissue distributes these drugs differently than lean tissue.
- Reversal agents must account for the same distribution differences to avoid residual paralysis in recovery.
Pro Tip: Ask your anesthesiologist before surgery whether they use ideal body weight or total body weight for each drug class. A confident, specific answer signals genuine bariatric experience.
How does the anesthesiologist manage anesthesia before and during surgery?
Anesthesia management for weight loss surgery begins weeks before the operating room. The preoperative anesthetic assessment for weight surgery is the foundation of every safety decision that follows.
-
Airway evaluation. The anesthesiologist grades airway difficulty using tools like the Mallampati score and neck circumference measurement. Patients with a Mallampati grade III or IV, or a neck circumference above 40 cm, are flagged for advanced airway strategies including video laryngoscopy.
-
OSA screening and CPAP review. Patients already using CPAP are instructed to bring their device to the hospital. Patients with undiagnosed OSA may be referred for a sleep study before surgery is cleared.
-
Comorbidity review. Hypertension, type 2 diabetes, and cardiovascular disease each affect anesthetic drug selection and monitoring intensity. The anesthesiologist coordinates with the surgeon and internist to adjust or pause medications like GLP-1 agonists and blood thinners before the procedure.
-
Toxicology screening. Preoperative toxicology screening uncovers undisclosed substance use that increases anesthetic requirements and delays recovery. Patients who screen positive require higher anesthetic doses but still achieve successful weight loss outcomes at one year, provided the team adjusts the plan accordingly.
-
Positioning for intubation. In the operating room, the anesthesiologist places the patient in the ramped position, aligning the ear to the sternal notch. This single positioning adjustment significantly improves the line of sight to the vocal cords and increases intubation success rates in obese patients.
Once the patient is under anesthesia, continuous monitoring drives every decision. The anesthesiologist tracks end-tidal CO2, oxygen saturation, blood pressure, and neuromuscular function in real time. For procedures like gastric bypass or gastric sleeve, the pneumoperitoneum created by laparoscopic gas insufflation further reduces lung compliance, requiring ventilator adjustments throughout the case.
Pro Tip: Tell your anesthesiologist about every supplement, herbal product, and over-the-counter medication you take. Substances like valerian, kava, and high-dose fish oil affect bleeding and sedation in ways that standard medication lists miss.
What postoperative care do anesthesiologists provide after weight loss surgery?
The anesthesiologist's responsibilities do not end when the surgeon closes the incision. Postoperative care by anesthesiologists covers the recovery room period and, in many centers, the first 24 hours of the hospital stay.
PONV affects 45.6% of bariatric surgery patients. That rate is higher than in most other surgical populations. PONV is not just uncomfortable. It prolongs hospital stays, increases dehydration risk, and strains fresh surgical staple lines in procedures like sleeve gastrectomy.
Anesthesiologists address PONV through several overlapping strategies:
- Prophylactic antiemetics given intraoperatively, typically ondansetron combined with dexamethasone, reduce PONV incidence significantly.
- Fluid management during surgery is calibrated to avoid both dehydration and fluid overload, since excess intraoperative fluid is a predictor of prolonged hospital stay beyond three days.
- Avoidance of nitrous oxide reduces PONV risk and is standard in most modern bariatric protocols.
- Early mobilization support through adequate pain control reduces nausea triggered by immobility.
Respiratory monitoring in the recovery room is equally critical. Patients with OSA face the highest risk of postoperative respiratory depression, especially when opioids are used for pain. Anesthesiologists prescribe CPAP continuation in recovery and set specific oxygen saturation thresholds that trigger escalation to a higher level of care.
Multimodal analgesia is the standard approach to postoperative pain in bariatric surgery. No single drug or technique works for every patient. Combinations of regional nerve blocks, acetaminophen, NSAIDs, and low-dose ketamine reduce opioid consumption while maintaining adequate pain control. Less opioid use means less respiratory depression, less nausea, and faster return to normal breathing.
How do modern anesthetic techniques improve outcomes in bariatric surgery?
The most significant recent advance in surgical anesthesiology in bariatric procedures is the shift toward opioid-free anesthesia (OFA). OFA replaces opioids with regional blocks and non-opioid systemic agents, addressing the respiratory risks that make opioids particularly dangerous in obese patients.
The erector spinae plane block (ESPB) is the regional technique with the strongest current evidence for laparoscopic bariatric surgery. A direct comparison shows how the leading approaches differ:
| Technique | Mechanism | Key Benefit | Primary Limitation |
|---|---|---|---|
| ESPB (erector spinae plane block) | Paravertebral nerve block via fascial plane | Reduces 24-hour morphine consumption significantly | Requires ultrasound skill and positioning |
| IV lidocaine infusion | Systemic anti-inflammatory and analgesic effect | Simpler to administer; no block needed | Less targeted; systemic side effects possible |
| Standard opioid-based anesthesia | Central pain suppression | Familiar protocol; widely available | Respiratory depression, PONV, delayed recovery |
ESPB reduces postoperative opioid needs more effectively than intravenous lidocaine in laparoscopic sleeve gastrectomy. That reduction matters because every milligram of opioid avoided lowers the risk of respiratory depression in a patient population already vulnerable to it.
Personalized protocol selection is the other defining feature of modern bariatric anesthesiology. Multimodal analgesia selection depends on patient health status, available hospital resources, and the anesthesiologist's specific expertise. A protocol that works well at a high-volume bariatric center in Tijuana may not be replicable at a general community hospital. This is one reason why choosing an accredited, high-volume bariatric center matters as much as choosing the right surgeon.
Key Takeaways
The anesthesiologist in weight loss surgery manages a three-phase process covering preoperative assessment, intraoperative monitoring, and postoperative recovery to protect patients from the specific risks that obesity creates.
| Point | Details |
|---|---|
| Obesity changes anesthesia fundamentally | Reduced lung capacity and difficult airways require specialized protocols, not standard general anesthesia. |
| Preoperative assessment is non-negotiable | OSA screening, toxicology testing, and airway grading directly shape the anesthetic plan and reduce intraoperative risk. |
| PONV affects nearly half of bariatric patients | Prophylactic antiemetics and careful fluid management shorten hospital stays and protect surgical staple lines. |
| Opioid-free anesthesia reduces key risks | ESPB and multimodal analgesia lower opioid consumption, respiratory depression, and recovery time. |
| Protocol personalization determines outcomes | No universal anesthetic plan exists; the best results come from centers with experienced bariatric anesthesiologists. |
What patients consistently underestimate about bariatric anesthesia
Most patients I speak with think of anesthesia as a single event. You go under, the surgeon operates, you wake up. That mental model is wrong, and it leads to real gaps in preparation.
Anesthesia in bariatric surgery is an integrated process. The decisions made six weeks before your procedure, including whether your OSA is treated, whether your blood pressure is controlled, and whether you disclose every substance you use, directly determine what happens in the operating room and recovery room. I have seen patients surprised by extended recovery room stays because undisclosed cannabis use shifted their anesthetic requirements in ways the team had not planned for. Toxicology screening exists to close that gap, not to judge you.
The other thing patients consistently underestimate is PONV. Nearly half of bariatric patients experience it. It is not a minor inconvenience. Severe nausea after a sleeve gastrectomy or gastric bypass procedure strains the new anatomy in ways that can affect healing. Ask your anesthesiologist specifically what their PONV prevention protocol includes. If the answer is vague, that tells you something.
The anesthesiologist is not a background figure. They are the person most responsible for keeping you alive and stable while the surgeon works. Choosing a center where the anesthesiologist has specific bariatric experience is not a luxury. It is a safety requirement.
— Ariel
Choosing a bariatric center with strong anesthesiology care
Selecting the right surgical center means evaluating the entire perioperative team, not just the surgeon's credentials. Anesthesiology expertise, PONV protocols, and postoperative respiratory monitoring are all part of what separates a high-quality bariatric program from a general surgical center that occasionally performs weight loss procedures.
Weightlosssurgeryguide evaluates bariatric providers in Tijuana specifically on these criteria. The 2026 provider rankings include centers with internationally accredited anesthesiology teams, documented opioid-free protocols, and structured postoperative monitoring programs. US patients can access this level of care at 60–75% less than domestic pricing without sacrificing the safety standards that bariatric anesthesia demands. Review the rankings to compare centers by procedure type, accreditation, and patient outcomes before you commit to a program.
FAQ
What does an anesthesiologist do during weight loss surgery?
The anesthesiologist manages airway access, drug dosing, and vital sign monitoring throughout the procedure. They also lead postoperative respiratory and pain management to reduce complications specific to obese patients.
Why is anesthesia more risky for bariatric surgery patients?
Obesity reduces functional residual lung capacity by 30–50% and increases the likelihood of difficult airway management by 3–5 times. These factors, combined with high OSA prevalence, make bariatric anesthesia significantly more complex than standard general anesthesia.
What is opioid-free anesthesia and is it used in bariatric surgery?
Opioid-free anesthesia replaces opioids with regional nerve blocks like ESPB and non-opioid systemic agents. It is increasingly standard in bariatric surgery because it reduces respiratory depression and PONV in patients already at elevated risk for both.
How does the anesthesiologist prevent nausea after bariatric surgery?
Anesthesiologists use prophylactic antiemetics like ondansetron and dexamethasone, avoid nitrous oxide, and manage intraoperative fluids carefully. PONV affects 45.6% of bariatric patients, making prevention a primary focus of postoperative anesthetic care.
What should I tell my anesthesiologist before weight loss surgery?
Disclose all medications, supplements, herbal products, and any substance use including cannabis and alcohol. Undisclosed substance use increases anesthetic requirements and can delay recovery, as preoperative toxicology screening consistently demonstrates.