Surgical Weight Loss Definition: What You Need to Know
Published June 29, 2026

Surgical Weight Loss Definition: What You Need to Know
Surgical weight loss, clinically known as metabolic and bariatric surgery, is defined as procedures that alter the stomach and/or small intestine to help patients with obesity achieve significant, sustained weight loss when diet, exercise, and medication have not worked. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) specifies that surgery is typically indicated for patients with a BMI above 35 kg/m², or above 30 kg/m² with obesity-related conditions such as type 2 diabetes, hypertension, or sleep apnea. These procedures do far more than shrink the stomach. They reprogram the hormonal signals that control hunger, satiety, and blood sugar, making surgical weight loss a metabolic intervention as much as a physical one.
What is the surgical weight loss definition and who qualifies?
Metabolic and bariatric surgery targets the root biology of obesity, not just caloric intake. By altering the digestive tract, these procedures change how the body processes food and regulates appetite hormones. That distinction matters because it explains why surgery produces results that diet alone rarely achieves long term.
Patient selection follows clear clinical criteria. A BMI above 35 kg/m² qualifies most patients regardless of other conditions. A BMI between 30 and 35 kg/m² qualifies when obesity-related comorbidities are present. Conditions that commonly meet this threshold include type 2 diabetes, obstructive sleep apnea, nonalcoholic fatty liver disease, and high blood pressure.
Approximately 260,000 people undergo these surgeries annually in the United States, representing roughly two thirds of global bariatric surgical volume. That scale reflects both the prevalence of obesity and the growing clinical confidence in surgery as a durable treatment. Weightlosssurgeryguide covers the full range of surgical weight loss options available to patients considering this path.
What are the main types of weight loss surgery?
Four procedures account for the vast majority of bariatric surgeries performed today. Each works through a different combination of restriction, malabsorption, and hormonal change.
| Procedure | Primary Mechanism | Reversible? | Average Total Weight Loss at 60 Months |
|---|---|---|---|
| Sleeve gastrectomy | Restriction + hormone change | No | ~23% total body weight |
| Roux-en-Y gastric bypass | Restriction + mild malabsorption | Rarely | ~26% total body weight |
| Biliopancreatic diversion with duodenal switch | Restriction + significant malabsorption | No | ~38% total body weight |
| Adjustable gastric banding | Restriction only | Yes | Lowest of the four |
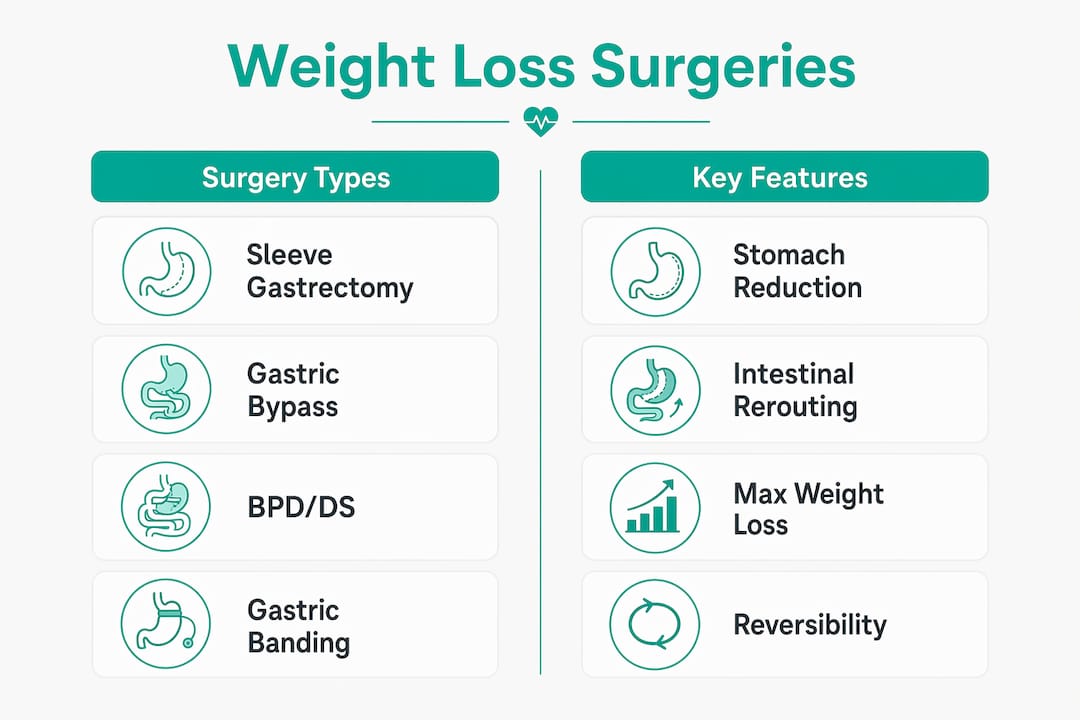
Sleeve gastrectomy removes roughly 80% of the stomach, creating a narrow tube. The reduced stomach size limits food intake, and the removal of the fundus lowers ghrelin production, which directly reduces hunger signals.

Roux-en-Y gastric bypass creates a small stomach pouch and reroutes the small intestine. Food bypasses most of the stomach and the upper small intestine, reducing both capacity and nutrient absorption. It consistently produces larger weight loss than banding but carries higher early postoperative complication rates.
Biliopancreatic diversion with duodenal switch (BPD/DS) is the most aggressive option. It produces the highest average weight loss of any procedure but also carries the highest risk of vitamin and protein malnutrition. Careful patient selection and lifelong supplementation are not optional with BPD/DS. They are mandatory.
Adjustable gastric banding places an inflatable band around the upper stomach to create a small pouch. It is the only fully reversible option, but outcomes are consistently lower than the other three procedures, and revision rates are high.
How does surgical weight loss work biologically?
The old framework classified bariatric surgery as either restrictive or malabsorptive. That model is now outdated. Modern classification recognizes that surgery reprograms neurohormonal pathways controlling hunger, satiety, and glucose regulation. The physical changes are the mechanism, not the full explanation.
After surgery, levels of GLP-1 (glucagon-like peptide 1) and peptide YY rise sharply. Both hormones signal fullness to the brain and slow gastric emptying. GLP-1 also stimulates insulin release from the pancreas. This is why diabetes remission can occur within days of gastric bypass, long before significant weight loss has happened. The hormonal shift precedes the scale change.
Ghrelin, the primary hunger hormone, drops significantly after sleeve gastrectomy because the ghrelin-producing cells in the fundus are removed. Patients report a genuine reduction in appetite rather than just a physical inability to eat large portions. The gut microbiome also shifts post-surgery, with changes in bacterial populations that appear to improve insulin sensitivity and energy metabolism independently of caloric restriction.
Pro Tip: If you are comparing surgical options, ask your surgeon specifically how each procedure affects GLP-1 and ghrelin levels. Those hormonal profiles predict long-term hunger management as much as the anatomy does.
What are the benefits and expected outcomes of weight loss surgery?
Weight loss after bariatric surgery follows a predictable pattern. Most patients lose the majority of their weight within the first 6–12 months post-surgery, with slower loss or weight stabilization afterward. Excess body weight loss ranges from 50–70% depending on the procedure, with gastric bypass generally producing the largest results.
The benefits extend well beyond the scale. Obesity-related comorbidities improve dramatically in most patients:
- Type 2 diabetes: Remission rates are high, particularly after gastric bypass and BPD/DS, often within weeks of surgery.
- Hypertension: Blood pressure normalizes in a majority of patients, frequently reducing or eliminating medication needs.
- Obstructive sleep apnea: Symptoms resolve or improve significantly as excess weight decreases pressure on the airway.
- Joint pain and mobility: Reduced mechanical load on knees and hips produces rapid functional improvement.
Metabolic surgery reduces mortality risk associated with cardiovascular disease, type 2 diabetes, and certain cancers. That mortality benefit is one of the most clinically significant arguments for surgery in high-risk patients. Weight loss alone does not fully account for it. The hormonal and microbiome changes post-surgery contribute independently to improved metabolic health.
Postoperative monitoring is structured and consistent. Patients are typically seen every 4–12 weeks during the first six months, then every 6–12 months for long-term maintenance. That schedule exists because the first year is when nutritional deficiencies and behavioral patterns are most likely to emerge.
What are the long-term requirements after surgical weight loss?
Surgery is not a one-time fix. Long-term success depends on a set of lifelong commitments that begin the day of discharge and never end.
-
Lifelong nutritional supplementation. Malabsorptive procedures create real risk of deficiencies in iron, vitamin B12, calcium, vitamin D, and folate. Protein-calorie malnutrition risk is highest after BPD/DS and can develop silently without consistent supplementation protocols. Missing supplements for weeks is not a minor lapse. It can lead to chronic, severe complications.
-
Psychological support and behavioral monitoring. Patients can circumvent the surgery's restrictive effects by consuming calorie-dense liquids, which pass through the stomach pouch without triggering satiety. This is one of the most common drivers of weight regain. Cognitive behavioral therapy is widely recommended post-surgery to address this pattern and other disordered eating behaviors.
-
Structured follow-up care. Postoperative monitoring every 4–12 weeks for the first six months, then every 6–12 months, is the clinical standard. These visits track weight, nutritional labs, blood pressure, and metabolic markers. Skipping follow-up appointments is the single most predictable path to poor long-term outcomes.
-
Dietary behavior change. Eating slowly, chewing thoroughly, avoiding high-sugar foods, and separating liquids from meals are not temporary post-op rules. They are permanent habits that protect the surgery's results.
-
Physical activity. Regular movement accelerates weight loss in the first year and is critical for preserving lean muscle mass during rapid weight reduction.
Pro Tip: Before choosing a surgeon or facility, ask for their protocol on long-term follow-up care. A program without a structured multidisciplinary follow-up plan is a red flag, regardless of how low the price is.
Long-term surgical success depends on multidisciplinary follow-up that integrates nutritional, psychological, and medical care. No single element is optional. Patients who engage with all three components consistently outperform those who treat surgery as a standalone event.
Key Takeaways
Surgical weight loss is a metabolic intervention that works through hormonal reprogramming, not just physical restriction, and requires lifelong commitment to nutrition, behavior, and follow-up care to succeed.
| Point | Details |
|---|---|
| Clinical definition | Metabolic and bariatric surgery alters the digestive tract to produce sustained weight loss in patients with obesity. |
| Procedure differences | BPD/DS produces the highest weight loss (~38%) but carries the greatest malnutrition risk; sleeve and bypass are more common. |
| Hormonal mechanism | GLP-1 and peptide YY rise post-surgery, driving diabetes remission and appetite reduction independent of weight loss. |
| Expected outcomes | Patients lose 50–70% of excess body weight, with most loss occurring in the first 6–12 months post-surgery. |
| Lifelong requirements | Nutritional supplementation, psychological support, and structured follow-up care are permanent, not temporary. |
What I've learned about surgical weight loss that most articles miss
Most articles about bariatric surgery focus on the procedure itself. The operation takes one to three hours. The real work takes years.
The biggest misconception I see is that patients treat surgery as the finish line. They research procedures, compare surgeons, prepare for the operation, and then expect the weight to handle itself. What actually determines long-term success is everything that happens after the patient leaves the hospital. The hormonal changes are real and powerful. But they are not permanent shields against poor habits.
The rapid diabetes remission that happens within days of gastric bypass is genuinely remarkable. It shows that surgery acts on metabolic disease at a biological level that no diet can replicate. That should raise the status of bariatric surgery in how patients and physicians think about obesity treatment. It is not a last resort. For many patients, it is the most evidence-based option available.
What I find underreported is the psychological dimension. Patients who consume high-calorie liquids post-surgery are not failing because they lack willpower. They are navigating a behavioral pattern that the surgery's anatomy does not block. Cognitive behavioral therapy is not an add-on. It is part of the treatment. Programs that skip it are delivering an incomplete intervention.
The shift in how the field classifies these procedures, from restrictive and malabsorptive to metabolic, reflects a more honest understanding of what surgery actually does. Patients deserve to understand that framing before they make a decision. Surgery changes your biology. That is its power and its responsibility.
— Ariel
Weightlosssurgeryguide: a resource for your surgical weight loss decision
Understanding the definition of surgical weight loss is the first step. Choosing the right provider is the one that determines your outcome.
Weightlosssurgeryguide evaluates accredited bariatric surgery providers in Tijuana for US patients, with verified rankings based on safety, credentials, and patient outcomes. US patients typically save 60–75% compared to domestic pricing while accessing internationally accredited care. The 2026 provider rankings cover sleeve gastrectomy, gastric bypass, BPD/DS, and revisional procedures, with transparent cost and accreditation data for each facility. If you are weighing surgery against medication-based options, the GLP-1 vs. bariatric surgery comparison page breaks down long-term outcomes, costs, and clinical evidence side by side.
FAQ
What is the clinical definition of surgical weight loss?
Surgical weight loss, or metabolic and bariatric surgery, is defined as procedures that alter the stomach and/or small intestine to help patients with obesity achieve sustained weight loss when non-surgical methods have failed. It is indicated for patients with a BMI above 35 kg/m², or above 30 kg/m² with obesity-related comorbidities.
How does weight loss surgery work beyond restricting food intake?
Surgery triggers hormonal changes, including rises in GLP-1 and peptide YY, that reduce hunger and improve insulin sensitivity. These metabolic effects explain why type 2 diabetes can go into remission within days of gastric bypass, before significant weight loss occurs.
Is surgical weight loss safe?
Bariatric surgery is considered safe when performed by credentialed surgeons in accredited facilities, with complication rates comparable to other common abdominal procedures. Long-term safety depends on lifelong nutritional supplementation and structured follow-up care to prevent deficiencies and weight regain.
Which type of weight loss surgery produces the most weight loss?
Biliopancreatic diversion with duodenal switch produces the highest average total weight loss at approximately 38% of total body weight at 60 months. It also carries the highest risk of nutritional deficiencies and requires the most rigorous lifelong supplementation.
How long does it take to lose weight after bariatric surgery?
Most patients lose the majority of their excess weight within the first 6–12 months post-surgery. Weight loss slows or stabilizes after that period, and long-term maintenance depends on diet, activity, and consistent follow-up care.